
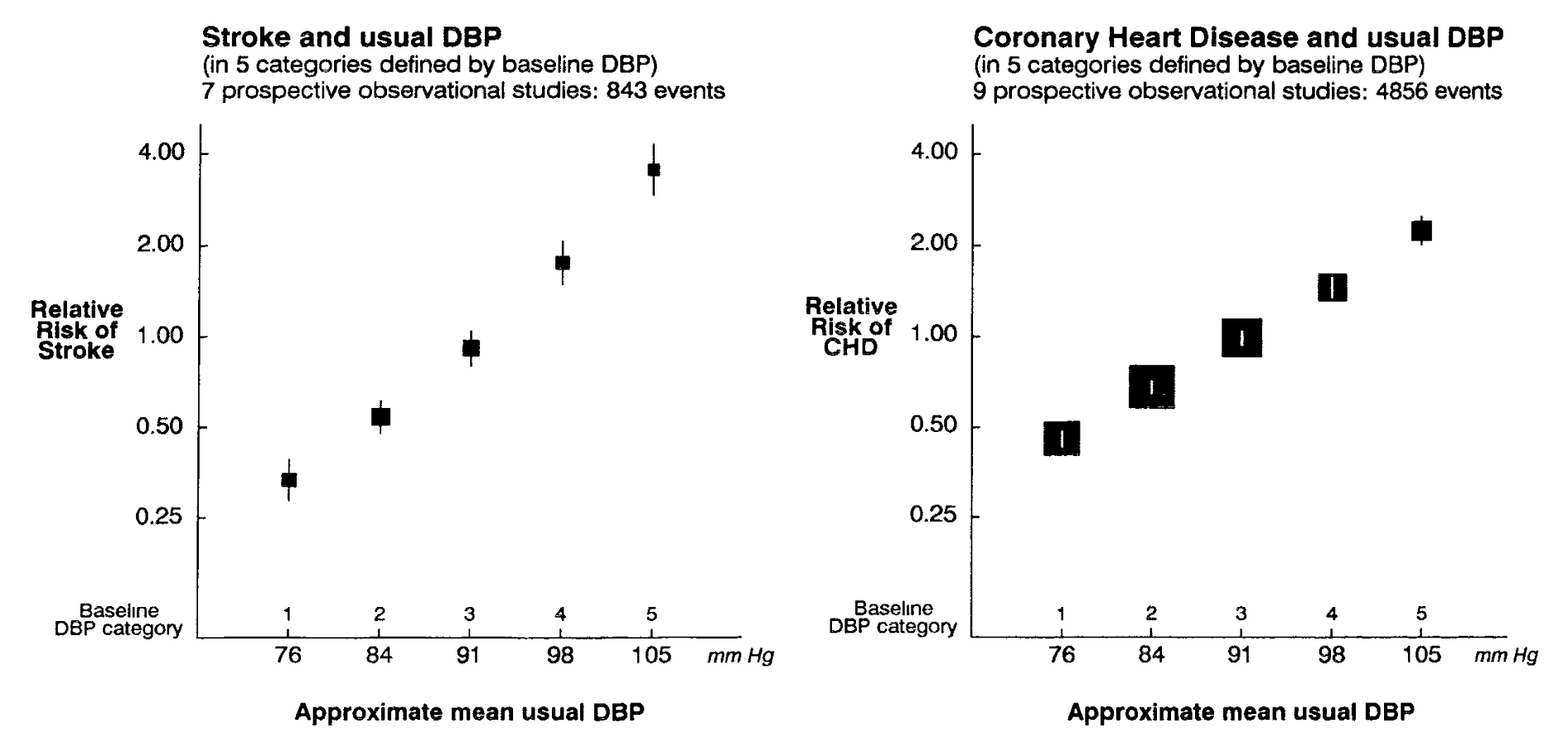
In relation to the relationship between hypertension and CVD, the data is unequivocal: hypertension profoundly increases risk for CVD events and mortality, and this relationship is linear and exhibits a strong dose-response.
MacMahon et al. (Lancet. 1990;335(8692):765–74) showed that the relative risk of stroke and coronary heart disease was 10-12 and 5-6 times greater, respectively in the highest diastolic blood pressure categories, compared to the lowest.
The link between hypertension and CVD, in particular stroke and coronary heart disease, satisfies every element of the Bradford-HIll criteria.
The association is strong, consistent, specific, temporal, i.e, hypertension precedes disease, graded, i.e., shows a clear – in this case linear – dose-response.
There is clear biological plausibility from experimental evidence, the overall body is evidence is coherent, and risk is reversible with reductions in hypertension.
But what about other potential health effects of high sodium intake and the broader scope of high sodium health risks?
Gastric Cancer Risk in the INTERSALT Cohorts
One of the first major international studies investigating salt intake and health outcomes across populations was the INTERSALT study.
INTERSAL used repeated measurements of 24 h urinary sodium in 10,079 participants in 52 research centres across 32 countries.
Using multiple 24 h urinary sodium collections provided the most robust assessment of sodium available to nutrition research.
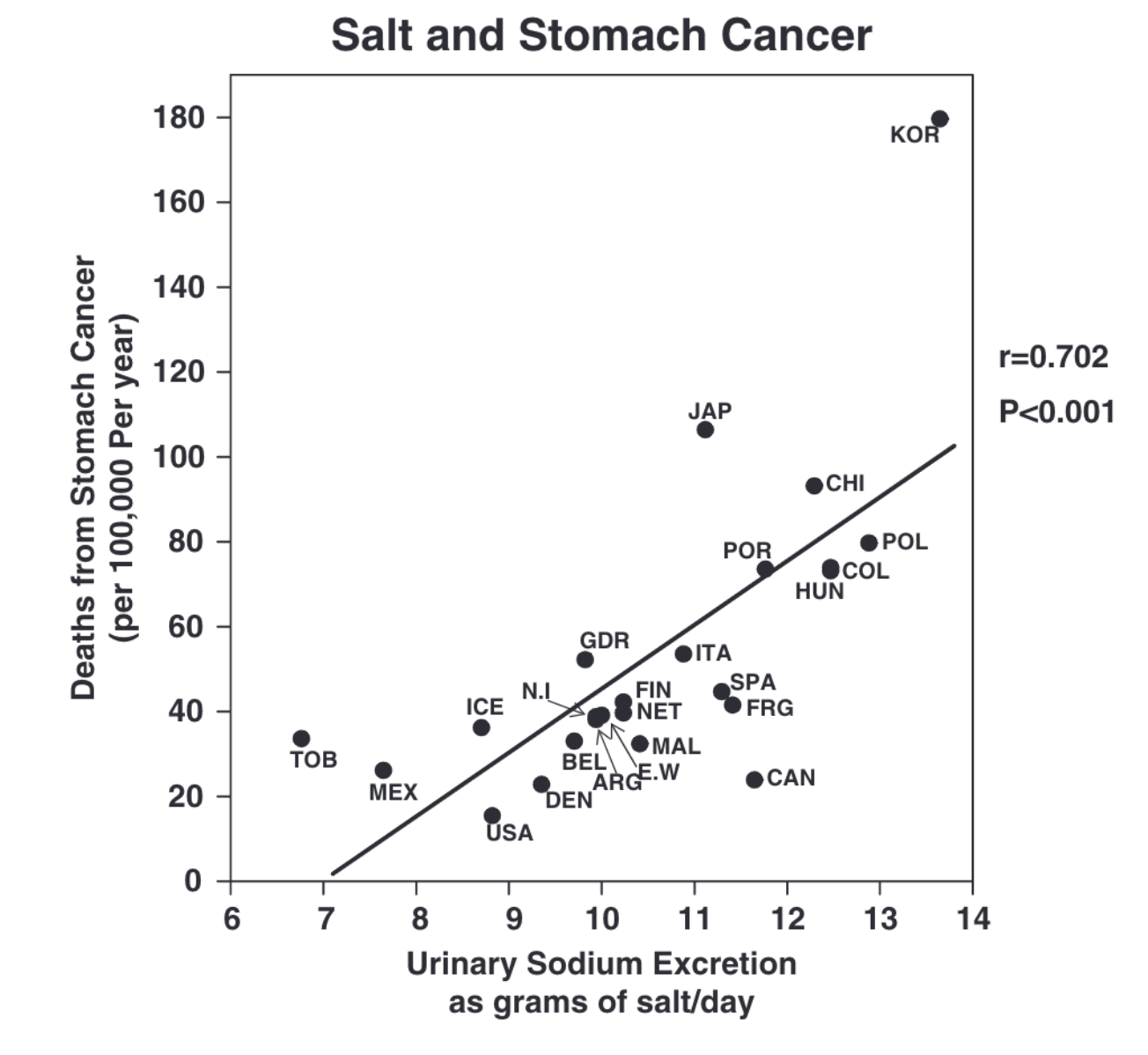
In addition to cardiovascular outcomes, INTERSALT was one of the first studies to observe a strong correlation between sodium and another outcome: gastric [stomach] cancer, a key finding in the study of diet and gastric cancer.
This association was observed (see figure, below) in a study based on data from 39 cohorts in 24 countries, in sodium correlated strongly with stomach cancer mortality (r = 0.702).
How Does Salt/Sodium Influence Gastric Cancer Risk?
As you may expect, the proposed mechanisms and related experimental evidence for gastric cancer differ from CVD.
Perhaps the mechanism which has attracted the most interest to date relates to H.pylori infection, a type of bacteria which itself is one of the leading risk factors for stomach cancer.
H.pylori colonises the stomach when given the opportunity to infect, and there is experimental evidence which shows that H.pylori causes more damage to epithelial cells in the stomach in the presence of high salt levels.
The epidemiology of salt has also shown interactions between salt and N-nitroso compounds [often found in processed meats] on the risk of stomach cancer, highlighting a complex mechanism within diet and gastric cancer.
Mechanistic research also shows that high salt levels reduce the viscous layer protecting the stomach, exposing the stomach lining to carcinogenic effects from N-nitroso compounds.
There is animal evidence that sodium chloride increases expression for certain genes which may promote gastric mucosal cell proliferation, potentially resulting in chronic gastritis.
Animal studies indicate that high salt intakes may result in reduced gastric blood flow and increased inflammatory pathways associated with chronic atrophic gastritis.
The addition of N-nitroso carcinogenic compounds in such a high-salt gastric environment appears to rapidly generate carcinogenesis in the stomach.
So overall, salt appears to act as a moderating factor to carcinogenic processes in the stomach, rather than exerting direct carcinogenic effects itself.
This may be through several mechanisms, including:
- Augmenting the adverse effects of H.pylori infection;
- Reducing protection of the gastric mucosa and;
- Influencing blood flow, inflammatory, and immune pathways and promoting gastritis.
In both 2) and 3), it appears that there is significant interaction with exposing the stomach to the carcinogenic effects of N-nitroso compounds.
Where Does the Evidence Stand Today?
The most recent synthesis of evidence in this area was published in 2021 by Wu et al. (Front Nutr. 2021; 8: 801228), contributing to the growing body of literature on diet and gastric cancer.
The study was a meta-analysis of prospective cohort design with participants free from gastric cancer at inclusion.
The exposures of interest were total dietary salt intake, picked foods, salted fish, processed meat, and miso soup.
The outcomes of interest were gastric cancer incidence and/or mortality. The analysis compared the highest vs. lowest levels of intake for each exposure.
Compared to the lowest salt intake, high total dietary salt intake was associated with a 25% [95% CI, 10% to 41%] higher risk of gastric cancer.
Of specific foods, high pickled foods intake was associated with a 28% [95% CI, 5% to 57%] higher risk of gastric cancer.
The association was stronger for gastric cancer mortality [~89% higher risk] compared to incidence [~14% higher risk].
Regional and Sex Differences in the Association
It is interesting to note the striking differences in relation to geographic region and sex associated with gastric cancer risk.
For example, in the Wu et al. study, cohorts in Asia exhibited a 32% higher gastric cancer risk, while there was no significant association in US/European cohorts. In addition, the association was significant for men, but not women.
However, hese findings are not novel.
In fact, if we go right the way back to the INTERSALT study referred to above, similar findings were observed in that study in the late 1980s.
In INTERSALT, men exhibited a higher risk for gastric cancer than women, and participants in Japan, Korea, and China exhibited higher risk compared to the US and/or several European cohorts.
Other studies have shown this regional distinction. For example, a 2012 meta-analysis by Ge et al. (Gastroenterol Res Pract. 2012:2012:808120) showed no significant association between high salt intake and gastric cancer in European cohorts, but 27% higher odds in Asian cohorts.
Confining the analysis to cohorts in Japan only, the Japanese cohorts showed 3-fold higher odds for gastric cancer.
Another 2012 meta-analysis by D’Elia et al. (Clin Nutr. 2012;31(4):489–98) also showed a nearly 3-fold higher risk in Japanese cohorts, but no significant associations in US/European cohorts.
These findings remain to be fully explained but may relate to factors like higher habitual salt intakes, specific foods/condiments [i.e., soy sauce], and higher prevalence of other risk factors [H.pylori, smoking, alcohol], all of which complicate the relationship between diet and gastric cancer.
How Consistent is the Association?
As it happens, salt was linked to gastric cancer as early as the 1950s in Japan.
And the geographic differences in gastric cancer risk generally, and in relation to high salt intake, are consistent findings in this research.
The interaction between high sodium intakes may explain, at least in part, associations of higher gastric cancer risk in Asian cohorts.
For example, it has been noted that while the prevalence of H.pylori in both US and Japanese adults aged 20 years is <20%, by age 40-50 the prevalence in US and Japanese adults has shifted to 40% compared to 80%, respectively.
Factoring in two more risk factors – age and salt – may mean that salt, age, and H.pylori all interact in the stomach to pose a higher risk of cancer.
Nevertheless, I am not sure I would bank on where I live determining the potential effect of high salt intakes on gastric cancer risk alone.
Unfortunately, the major limitation of this area of research is the lack of any standardised quantification for the levels of sodium intake, and intakes of sodium-rich foods, associated with risk, making it difficult to fully assess high sodium health risks.
This makes it difficult to compare to, for example, the recommendations for cardiovascular health, which typically are for <5-6g/d salt [<2,000-2,400mg/d sodium].
It would appear prudent to assume, in the absence of any quantification yet concerning gastric cancer, that a similar threshold would suffice for risk reduction.
Yours in Science,
Alan
Learn with Us.
You’ll find our most comprehensive resources in the Alinea Nutrition Education Hub.
Our weekly Deepdive takes a take a forensic look at a recent study: you’ll understand the background, the findings, and the relevance of the study in the context of the wider literature.
Our bi-monthly video Research Lectures condense complex topics into a visual presentation for you to maximise your learning experience.
And Exclusive Articles from researchers and academics in the field of nutrition science provide insights and perspectives from the people producing the research.