
Polycystic Ovarian Syndrome [PCOS] is the most common endocrine disorder in women of reproductive age, with a prevalence rate of 5-10%.
However, some estimates may be nearer to 20% depending on the diagnostic criteria.
PCOS is driven by disturbances of the hypothalamic-pituitary-adrenal-ovarian [HPAO] axis.
At the hypothalamic and pituitary levels, gonadotropic dysfunction, i.e., dysfunction of hormones secreted by the pituitary gland that act on maturation and function of the ovaries, is characteristic of PCOS.
Increased gonadotropin-releasing hormone [GnRH] from the hypothalamus causes hypersecretion of luteinizing hormone [LH] from the pituitary.
Elevated LH stimulates the production of androgens by the ovaries.
Inadequate production of follicle-stimulating hormone [FSH] also contributes to anovulation in PCOS.
In women with PCOS, insulin levels also influence the production of androgens from the ovaries.
As a result of this HPAO-axis and insulin dysfunction, PCOS appears to be the leading cause of infertility in women, secondary to the loss of ovulatory cycles, making the connection between a pcos diet and fertility a key area of study.
Reproductive Risk in Women with PCOS
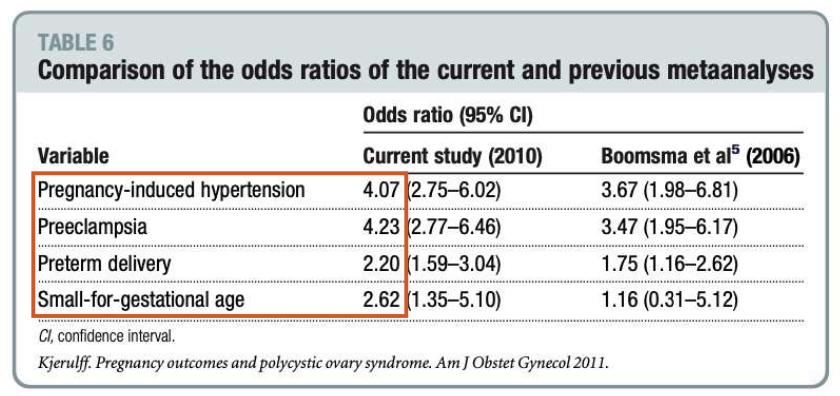
The table below, from Kjerulff et al. (Am J Obstet Gynecol. 2011 Jun;204(6):558.e1-6) illustrates the odds of adverse pregnancy outcomes in women with PCOS.
As you can see within the encapsulated red rectangle, the odds of pregnancy-induced hypertension and preeclampsia are 4-fold higher, while the odds of preterm delivery and small-for-gestational-age are 2-3-fold higher.
With PCOS phenotypes characterised by anovulation, longer menstrual cycle lengths of >35 days correlate with insulin resistance.
And up to 80% of women with anovulatory infertility have PCOS.
This extends to the risk of miscarriage, which is increased in women with PCOS whether their pregnancy was achieved spontaneously, or with assistance.
Can Diet or Supplements Help?
Given the interaction between metabolic and endocrine dysfunction in PCOS, it is plausible that certain dietary interventions may benefit for reproductive outcomes, which is the core focus of research into a pcos diet and fertility.
It is important to stress that the body of evidence for nutrition interventions in PCOS remains dominated by small trials, low statistical power, varying consistency in effects, and the size of those effects.
However, there are some take-home points we can derive from the evidence that does exist.
The first is weight loss, given the relationship between adiposity, insulin, and androgens in PCOS.
A Cochrane Review by Lim et al. (2019 Mar 28;3(3):CD007506) found that dietary and lifestyle interventions in women with PCOS resulted in an average of ~1.68kg weight loss.
However, this was related to an improved androgenic profile, i.e., higher sex hormone-binding globulin and lower testosterone levels.
Kazemi et al. (Adv Nutr. 2021 Feb 1;12(1):161-178) also reviewed the role of carbohydrate quality, i.e., low glycaemic index diets, and found low-GI diets improved metabolic and androgenic outcomes.
However, this was only in studies using energy-restricted diets, which makes it difficult to attribute any outcomes to the low-GI component.
An interesting study from Mehrabani et al. (J Am Coll Nutr. 2012 Apr;31(2):117-25) combined both low-carb and lower total fat with higher protein intake.
Their trial suggested that the greatest improvement in androgen levels and metabolic outcomes in PCOS may be observed with diets of both <35% total fat and <45% total carbohydrate.
What About Fertility Outcomes?
While the preceding research indicates that the overall hormonal profile may be improved with certain dietary interventions, does this translate into meaningful outcomes, specifically regarding a pcos diet and fertility?
Shang et al. (Front Endocrinol (Lausanne). 2021; 12: 735954) conducted a meta-analysis of dietary interventions for reproductive outcomes in PCOS.
To be included, the primary studies were required to be parallel-arm [where the intervention and comparison groups run at the same time], randomised controlled trials [RCTs].
They were also required to be dietary pattern interventions, rather than nutrient or supplement trials, and have reported on pregnancy rate and ovulation rate as outcomes.
Based on 12 trials with 740 participants, women in the dietary intervention groups had a 187% higher probability of pregnancy compared to women in the control groups.
In subgroup analysis, the increase in pregnancy rate was significant for the low-carb diets, and only for studies greater than 3 months in duration.
For the ovulation rate, which was based on three trials with 192 participants, women in the dietary intervention groups had a 30% higher probability of ovulation compared to women in the control groups.
In subgroup analysis, this improvement in ovulation rate was only observed in studies without calorie restriction, not with calorie restriction. This is consistent with the relationship between energy balance and ovulatory health in women.
It is important to consider the carbohydrate levels in the primary included studies; the lowest level on average was 25-30% of total carbohydrate intake. 4/7 included studies on low-carb diets had average levels of 40-50% carbohydrate.
What about the fat content of these diets? As most of these studies were conducted in China, total fat was never higher than 30% in any study.
Again, this is particularly relevant for PCOS because prior research suggests that the greatest diets of both <35% total fat and <45% total carbohydrate may produce more favourable endocrine improvements.
Thus, it is crucial to note that “low-carb” does not mean “no-carb” for PCOS, and does not equate to “high-fat” diets, either.
Recall also that this study stipulated the inclusion of dietary trials rather than supplement trials.
Thus, the meta-analysis did not include perhaps the most promising available supplemental option for women with PCOS, namely inositol.
Inositol exists in two forms; myo-inositol [MI] and d-chiro-inositol [DCI], both of which have distinct but complementary effects on PCOS; increasing insulin sensitivity and glucose tolerance, lower androgens, and menstrual cycle regularisation.
MI alone has been shown to benefit reproductive function in women with PCOS (Unfer et al. Endocr Connect. 2017 Nov; 6(8): 647–658).
Doses of ~4g/d have been shown to lead to spontaneous restoration of ovulation, improved oocyte quality, and reduction in insulin and androgens.
However, while DCI alone is not beneficial, combination supplementation of MI and DCI administered in the physiological ratio of 40:1 may ensure better clinical results.
Nordio et al. (Eur Rev Med Pharmacol Sci. 2019 Jun;23(12):5512-5521) showed that the combination of 4g/d MI:DCI restored ovulation with greater efficacy than other ratios.
Their group also demonstrated that the combination restored hormonal and metabolic function in women with PCOS earlier than MI alone.
What Can We Take From this Evidence?
Let’s put the outcomes from the meta-analysis in context.
First, the increased probability of pregnancy appears to be an enormous effect size, but the confidence intervals were very wide and indicated a lot of variability and imprecision in that finding.
Importantly, 74% of the statistical weight was derived from three studies, and each study had only ~40 participants in the intervention groups.
This is not to suggest that the finding of increased probability of pregnancy is invalid, merely to temper expectations with the size of the effect noted in this study; it is primarily based on three small trials and may be exaggerated.
Nevertheless, the study added to the research on available interventions for PCOS, indicating that dietary interventions, particularly those emphasising moderate carbohydrate intake, may also be a helpful adjuvant treatment, a vital component of any protocol targeting a pcos diet and fertility.
Of those available interventions, however, without doubt inositol may be considered a “frontline” nutritional supplement for women with PCOS.
The data on inositol was established before the publication of the Shang et al. meta-analysis, and is a low-hanging fruit as a supplement with a minimal risk profile.
At this juncture, we certainly have more consistent evidence that dietary interventions improve the hormonal aspects of PCOS, in particular elevated insulin and androgens.
And we understand the relationship between these risk factors and infertility in PCOS.
The Shang et al. meta-analysis suggests that the likelihood of meaningful clinical outcomes such as menstrual regularity and achieved pregnancy, may also be improved with diet, solidifying the evidence base for a pcos diet and fertility.
As always in this area, however, this is a “may”, and we still need some larger, better-designed trials to confirm the signal in the noise.
Yours in Science,
Alan
Learn with Us.
You’ll find our most comprehensive resources in the Alinea Nutrition Education Hub.
Our weekly Deepdive takes a take a forensic look at a recent study: you’ll understand the background, the findings, and the relevance of the study in the context of the wider literature.
Our bi-monthly video Research Lectures condense complex topics into a visual presentation for you to maximise your learning experience.
And Exclusive Articles from researchers and academics in the field of nutrition science provide insights and perspectives from the people producing the research.