
The core pathophysiology of type-2 diabetes [T2D] is the progressive decline, and eventual termination of function, in the capacity of the beta-cells [β-cells] of the pancreas to produce and secrete insulin.
While insulin resistance in peripheral tissues like skeletal muscle develops first, it is the loss of function of β-cells that characterises the progressive severity of the disease.
In this respect, diabetes is a spectrum of levels of glucose tolerance and insulin function, from impaired glucose tolerance [IGT] and pre-diabetes to a diagnosis of T2D.
Temporal Decline in Glucose Tolerance
The crucial point is that defects in glucose metabolism emerge often long before the diagnosis of a disease.
For example, people who have normal glucose tolerance that progress to IGT may have lost half of their β-cell function by the time they progress to IGT.
People with established IGT and an oral glucose tolerance test [OGTT] result near the cutoff for diagnosis of T2D, may have lost at least 80% of their β-cell function.
Roy Taylor’s research group have found using their very low-calorie diets for diabetes remission, that the capacity of β-cells to recover function may be contingent on the duration of the disease.
For example, there appears to be a greater probability of recovery of β-cells function in participants who are within 6 years of diagnosis.
The progressive deterioration in glucose tolerance and β-cell function indicates that time is a crucial factor in diabetes prevention.
While Taylor’s group have been focused on remission in patients already with T2D, large-scale diabetes prevention programs in several countries have focused on intervening at the earlier stages of IGT.
The Diabetes Prevention Trials
The major diabetes prevention trials have been conducted in the U.S., Finland, India, and China, providing the foundational data for most diabetes prevention studies.
Contrasting their results, particularly the long-term follow-up of the U.S. Diabetes Prevention Program [DPP] and Chinese Da Qing Study, provide some crucial insights into diabetes risk and mitigation.
In the DPP, participants with IGT and BMI >34kg/m2 were randomly assigned to either metformin, diet+exercise, or placebo.
Progression to TD2 was reduced by 58% in the lifestyle group, compared to the metformin group, over 3-years.
But what about at 15-years of follow-up?
There was no significant difference between lifestyle and metformin groups, although compared to the placebo group there remained a 27% lower T2D incidence in the lifestyle group.
In the metformin group, T2D incidence risk was 18% lower compared to the placebo group.
In the Chinese Da Qing IGT and Diabetes Study, 43% of the participants in the lifestyle intervention group progressed to a diagnosis of T2D, compared to 72% of the control [no diet or exercise] group.
At 20-years of follow-up, however, progression to T2D was 80% in the intervention group compared to 93% of controls.
Thus, while lifestyle interventions may yield greater prevention in the short-term, progression to T2D may still be high in the long-term.
Let’s think about the DPP long-term follow-up in more detail. The annual incidence of diagnosis over the entire 15-year study period was 7%, 5.7%, and 5.2% in the placebo, metformin, and lifestyle groups, respectively.
Over time, the significant difference between the lifestyle intervention and the metformin intervention groups that was evident during the initial 3-year DPP study dissipated, such that at 15 years of follow-up there was no significant difference between these two groups.
What could explain the erosion of effect over time in the diabetes prevention studies?
One clue lies in the DPP itself.
In a follow-up analysis of the respective contributions of weight loss, diet and exercise in the DPP lifestyle group, weight loss averaging 5kg over 3-years was the strongest factor associated with risk reduction, independent of exercise and diet composition, reinforcing the efficacy of weight loss for diabetes.
The figure, below, illustrates this point [“DDPOS” = DPP Outcomes Study]:
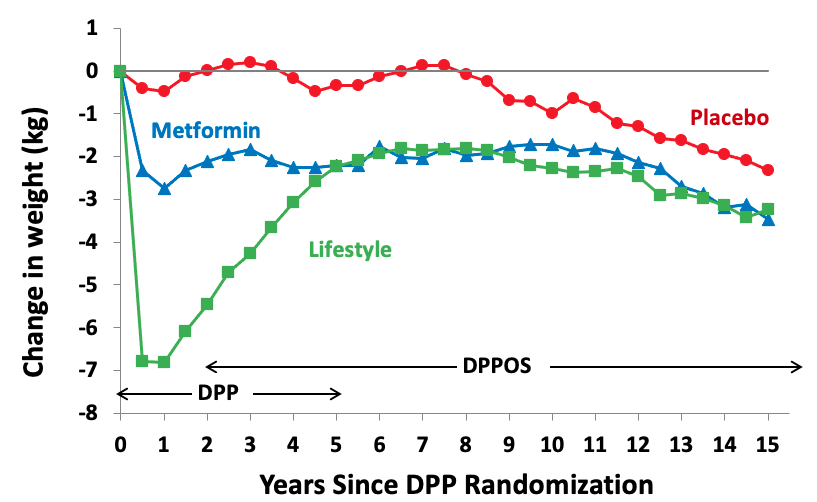
At the end of the first year of the DPP, mean weight loss was 0.4kg, 2.3kg, and 6.7kg in the placebo, metformin, and lifestyle groups, respectively.
By the end of the 3-year initial intervention, mean weight loss was 1.8kg and 4.2kg in the metformin and lifestyle groups, respectively.
By year 5 the difference in weight loss between metformin and lifestyle groups was abolished, and it remained similar for the duration of follow-up.
What the weight loss was facilitating, however, is more important: improved glycaemic control.
Over the first year of the intervention, the lifestyle group lost an average of 7% bodyweight, which correlated with significant reductions in fasting glucose.
However, by 3.5-years fasting glucose had returned to baseline levels in the lifestyle group and was associated with a weight reduction of just 4% below baseline at that point.
Cumulatively, the data suggests that a minimum threshold of weight loss and maintenance, a key principle of weight loss for diabetes, to prevent or delay progression from IGT to T2D.
What About the Other Diabetes Prevention Trials?
In the Finnish Diabetes Prevention Study [DPS], the incidence of progression to T2DM was reduced by 58% over a mean 3-years follow-up in subjects with IGT.
The magnitude of risk reduction was strikingly similar to the U.S. DPP over the same duration.
The reduction in risk in the DPS intervention group corresponded with an average weight loss over 3-years of 3.5kg vs. 0.8kg in the control group.
And, weight loss of 4.2kg over the first year of the trial coincided with the most significant drop in fasting glucose.
However, 10-year results from the DPS highlighted that relapses in weight corresponded with deteriorations in glucose tolerance and progression to T2D.
What Have We Learned?
Cumulatively, the data suggests weight loss and maintenance of 5kg or ~5% bodyweight is required to achieve improvements in glucose tolerance that are clinically meaningful for T2D risk reduction.
The various diabetes prevention trials, mirroring the broader conclusions of major diabetes prevention studies, have been fairly consistent in demonstrating a relationship between improved glucose tolerance and the degree of weight loss and maintenance.
A 2015 meta-analysis specifically focusing on glycaemic control in IGT found that diet and physical activity improve blood glucose regulation over an average follow-up period of 5-years.
However, the crucial learning from the diabetes prevention trials is that however, while diet and exercise may both be necessary, they may not alone be sufficient.
This is because the continued decline in β-cell function is the hallmark of the progression from IGT to T2D.
The diabetes prevention trials indicate that offsetting deteriorating β-cell function requires a certain threshold of weight loss to mitigate against IGT.
The limitations are the degree of weight loss required and the need to maintain that weight loss in the context of continued declining β-cell function.
While at present the interventions are effective, highlighting the success of these diabetes prevention studies, achieving long-term adherence in a real-world setting remains a challenge.
This evidence is another reason not to dichotomise weight loss into “good/bad”.
It is also another reason not to assume that it is easy for people to achieve.
Nevertheless, the diabetes prevention trials corroborate the crucial modifying effect of a minimum of 5% initial bodyweight loss, and the importance of diet and exercise in facilitating that risk reduction.
Yours in Science,
Alan
Learn with Us.
You’ll find our most comprehensive resources in the Alinea Nutrition Education Hub.
Our weekly Deepdive takes a take a forensic look at a recent study: you’ll understand the background, the findings, and the relevance of the study in the context of the wider literature.
Our bi-monthly video Research Lectures condense complex topics into a visual presentation for you to maximise your learning experience.
And Exclusive Articles from researchers and academics in the field of nutrition science provide insights and perspectives from the people producing the research.